The pilonidal disease most commonly occurs between the buttocks, close to the tailbone. This condition has been described since 1847.
The term pilonidal means hair-nest.
It can also occur in other areas such as beard, the armpit, the belly button and the web spaces of the hands (in barbers) and feet.
The condition results from a reaction to hairs embedded in the skin, commonly occurring in the cleft between the buttocks. The disease is more common in men than women and frequently occurs between puberty and age 40. It is also common in obese people and those with thick, stiff body hair.
Pilonidal disease is a spectrum of three conditions:
-acute pilonidal abscess,
-chronic pilonidal abscess or sinus,
-unhealed pilonidal surgical wound.
For many years, experts believed that this was a congenital condition. In 1946, Patty and Scarff challenged this theory and drew attention to the role of hair in the origin of this problem. Current evidence strongly indicates an acquired origin for pilonidal disease, with most infections being related to penetration of the skin by hair through small midline pits.
Example of pits and infection:

Where do these pits come from? Some people believe they are congenital while others believe them to be enlargement of hair follicles. These pits have sinus openings through which the hairs penetrate. Hirsutism in the buttock and perineal area appears to be associated with the development of pilonidal disease.
Management of the condition depends on the type of presentation.
Acute pilonidal abscess needs to be drained immediately once the diagnosis is made. The area should be kept shaved. Daily bath or shower will keep the area clean. Once healed, it may become necessary to excise the midline pits under local or general anaesthesia to prevent recurrence.
Treatment of chronic pilonidal abscess or sinus remains controversial as no one treatment has proved superior. The choices are:
-non-operative treatment with repeated phenol injections
-conservative excision of the sinus openings and midline pits
-laying open the sinus tract and stitch the skin margins to fibrous tissue (marsupialization)
-wide excision with or without different types of closures of the skin.
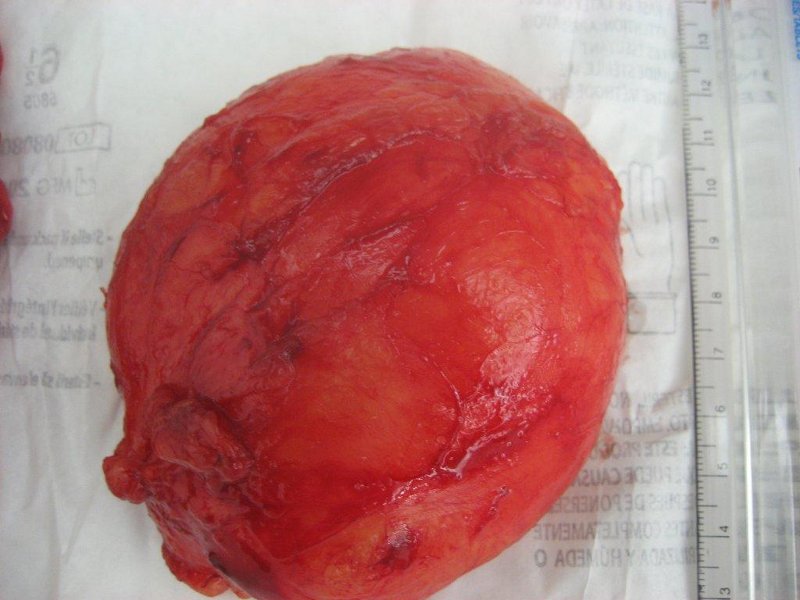
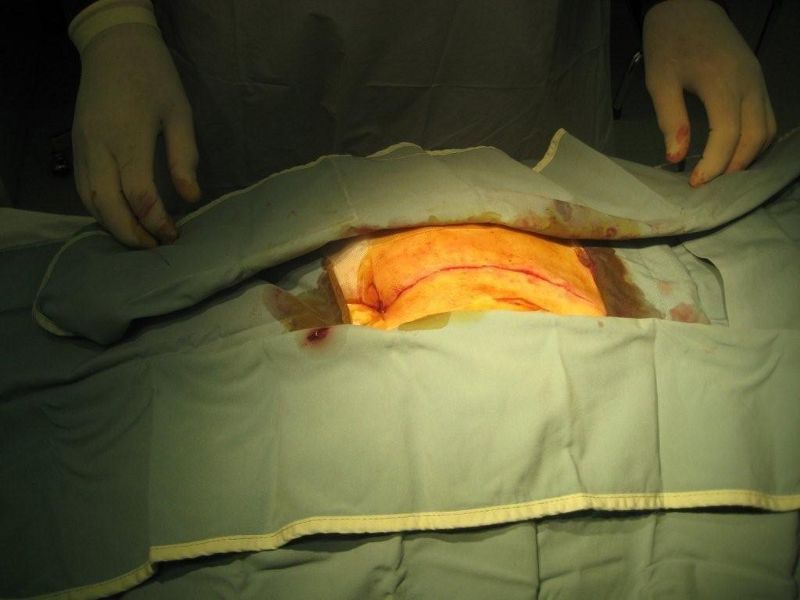
Example of wide excision:

The unhealed pilonidal surgical wound and recurrence of pilonidal disease after initial treatment is very common. Management of this problem can be very difficult. To start with, the unhealed wound should be curettaged to control the excessive granulation tissue (healing tissue which fills the wound), and the surrounding skin should be shaved weekly. The wound should be kept clean and dry with gauze. Strapping the buttocks apart may help prevent the continuous shearing movement during walking.
The wound may take six to eight weeks to heal. Quite often healing does not occur. Then a skin graft or some form of plastic flap may help the healing process.
If the wound can be closed, it will need to be kept clean and dry until the skin is completely healed.
If the wound must be left open, dressings or packing will be needed to help remove secretions and to allow the wound to heal from the bottom up.
After healing, the skin in the buttocks crease must be kept clean and free of hair. This is accomplished by shaving or using a hair removal agent every two or three weeks until age 30. After age 30, the hair shaft thins, becomes softer and the buttock cleft becomes less deep.
Overall, treating pilonidal disease should not be taken lightly as the results may be disappointing. There is no one good treatment which works for all patients with pilonidal disease




For more information visit:
-Another article on my website – Pilonidal Cyst
–American Society of Colon and Rectal Surgery
–Pilonidal disease support group
Start reading the preview of my book A Doctor's Journey for free on Amazon. Available on Kindle for $2.99!